2021 Prescription Drug Claim Form. Anthem has also.
 Syscalls In Charge Toll Fill Online Printable Fillable Blank Pdffiller
Syscalls In Charge Toll Fill Online Printable Fillable Blank Pdffiller
2021 Authorization to Disclose Protected Health Information PHI Form.
Blue shield of california prior authorization form pdf. Please include medical records when you. PDF Prescription prior authorization forms are used by physicians who wish to request insurance coverage for non-preferred prescriptions. Request or Refusal for Interpreter Service Form Arabic.
Coordination of Care and Treatment Summary Form. Find instructions for working in AuthAccel Blue Shield of Californias online authorization system. An Independent Licensee of the Blue Cross and Blue Shield Association MKT-148 Rev.
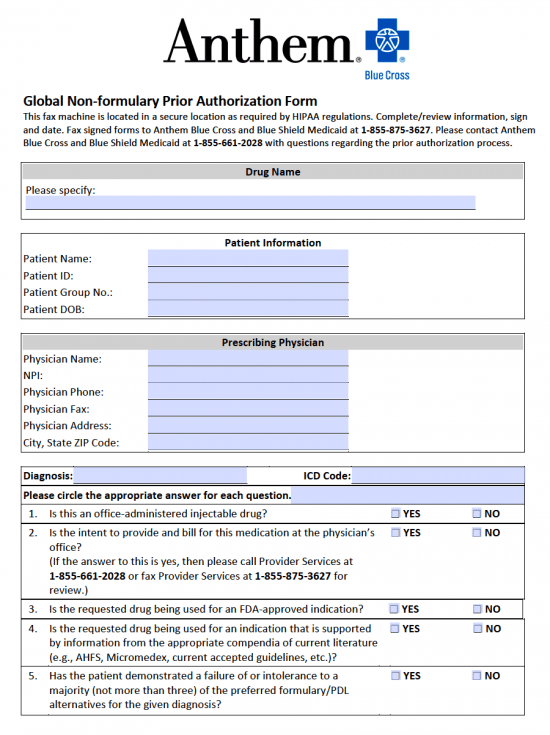
On the prior authorization form the person making the request must provide a medical rationale as to why the chosen medication is. 1-844-474-3345 For MediConnect Plan pharmacy requests please contact Anthem Blue Cross Cal MediConnect Plan Medicare-Medicaid Plan Customer Care at 1-855-817-5786. PDF The Anthem Blue Cross Blue Shield prior authorization form is what physicians will use when requesting payment for a patients prescription cost.
Services requiring prior authorization. Provider Forms Guides. A non-preferred drug is a drug that is not listed on the Preferred Drug List PDL of a given insurance provider or State.
To request prior authorization for treatment or for a drug you your doctor other prescriber or appointed representative need to contact Blue Shield of California Promise Health Plan and provide necessary clinical information. 2021 Medicare Part B vs. Cultural and Linguistic Referral Form.
Pharmacy Prior Authorization Center for Medi-Cal. 2021 Online Coverage Redetermination Request Form. 2021 CMS Appointment of Representative Form.
During this time you can still find all forms. A prior authorization is an approval review that Blue Shield of California Promise Health Plan conducts. 2021 Pharmacy Mail-Order Form.
GENERAL INFORMATION Patient Name Request Type please check one Prior Authorization. The form contains important information regarding the patients medical history and requested medication which Anthem will use to determine whether or not the prescription is included in the patients health care plan. Please fax the completed form to 716-887-8886.
2021 Mail-Order Physician New Prescription Fax Form. Chart notes or lab data to support the prior authorization or step therapy exception. Specialist as primary care provider request form.
Request to Resolve Provider Negative Balance. Request or Refusal for. Anthem Blue Cross of California Services Requiring Prior Authorization July 1 2013 - Effective August 1 2013 Page 2 of 8 Services Requiring Prior Authorization.
If authorization was not obtained prior to the service being rendered the service will likely be reviewed for medical necessity at the point of claim. Health insurance can be complicatedespecially when it comes to prior authorization also referred to as pre-approval pre-authorization and pre-certification. All forms are printable and downloadable.
Request a medical authorization PDF 329 KB View medical authorization status PDF 272 KB. Interpreter Services Attendance Verification Form. Provider Demographic Change Form Please submit this form to our Corporate Provider File Department when adding additional office locations to your practice or if your practice moves from its current location.
Once completed you can sign your fillable form or send for signing. Weve provided the following resources to help you understand Anthems prior authorization process and obtain authorization for your patients when its required. Blue Cross Blue Shield of Rhode Island is an independent licensee of the Blue Cross and Blue Shield Association.
We are currently in the process of enhancing this forms library. Fill Online Printable Fillable Blank Outpatient Treatment Authorization Request Blue Shield of California Form Use Fill to complete blank online BLUE SHIELD OF CALIFORNIA pdf forms for free. 5-2016 SUBMISSION INSTRUCTIONS GENERAL PRESCRIPTION DRUG COVERAGE AUTHORIZATION REQUEST FORM This form is for authorization of prescription drug benefits only and must be COMPLETELY filled out.
Please fill out the Prescription Drug Prior Authorization Or Step Therapy Exception Request Form and fax it to 877 327-8009. Medical Meals Referral Form. Download and print commonly requested forms for prior authorizations coverage determination requests referrals screenings enrollment for electronic claims submission and remittance advices and more.
Please fill out all applicable sections on both pages completely and legiblyAttach any additional documentation that is important for the review eg. The drug specific criteria and forms found within the Searchable lists on the Drug List Search tab are for informational purposes only to assist you in completing the Prescription Drug Prior Authorization Or Step Therapy Exception Request Form if they are helpful to you. Easily find and download forms guides and other related documentation that you need to do business with Anthem all in one convenient location.
All trademarks unless otherwise noted are the property of Blue Cross Blue Shield of Rhode Island or the Blue Cross and Blue Shield Association. Behavioral Health Treatment Authorization Request PDF 99 KB Community Based Adult Services CBAS Inquiry PDF 242 KB Community Based Adult Services. Prior authorization for the services listed below is highly recommended.
Blue Shield of California providers. For more information on obtaining prior authorization review refer to your provider manual. Page 2 of 2 Revised 122016 PRESCRIPTION DRUG PRIOR AUTHORIZATION OR STEP THERAPY EXCEPTION REQUEST FORM Patient Name.
Monday to Friday 7 am. Blue Shield Medicare Non-Formulary Exception and Quantity Limit Exception PDF 129 KB Prior AuthorizationCoverage Determination Form PDF 136 KB Prior. Providers serving Blue Shield of California Promise Health Plan members may check status of submitted prior authorization requests using the online tools.