On a non-color printout Required fields will appear. All items must be completed unless otherwise noted in these instructions.
Https Learn Medi Cal Ca Gov Warehouse Coursematerials Lms Medi Cal Cms1500 Bb 1 Pdf
Enter the amount due which may be a copayment a copayment and deductible or an amount due after other insurance applied all contractual reductions.
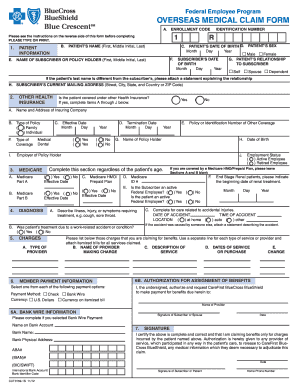
Cms 1500 claim form instructions. The CMS-1500 claim form has space for physicians and suppliers to provide information on other health insurance. 7500 Security Boulevard Baltimore MD 21244. Module Objectives Introduce general CMS-1500 claim form billing guidelines.
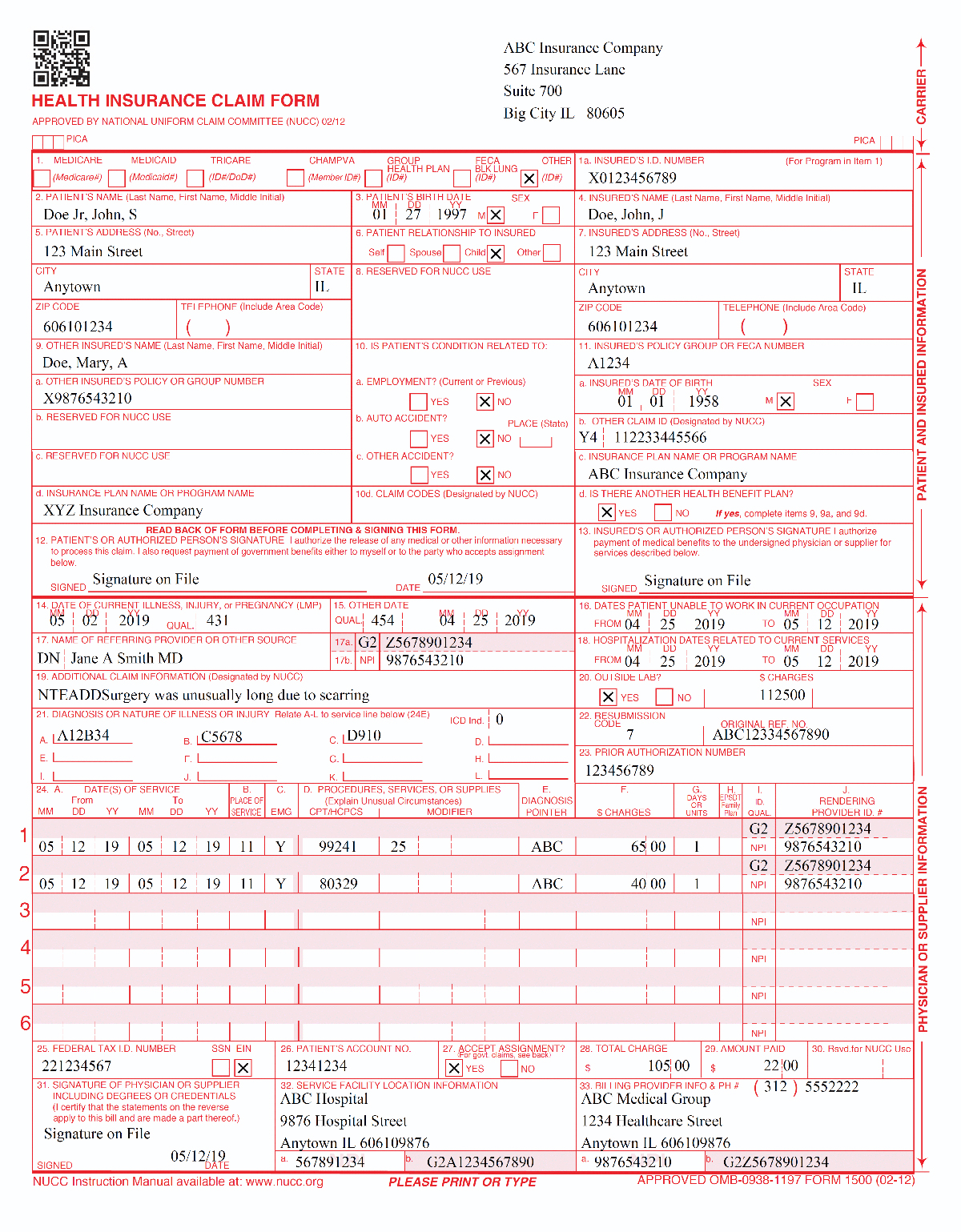
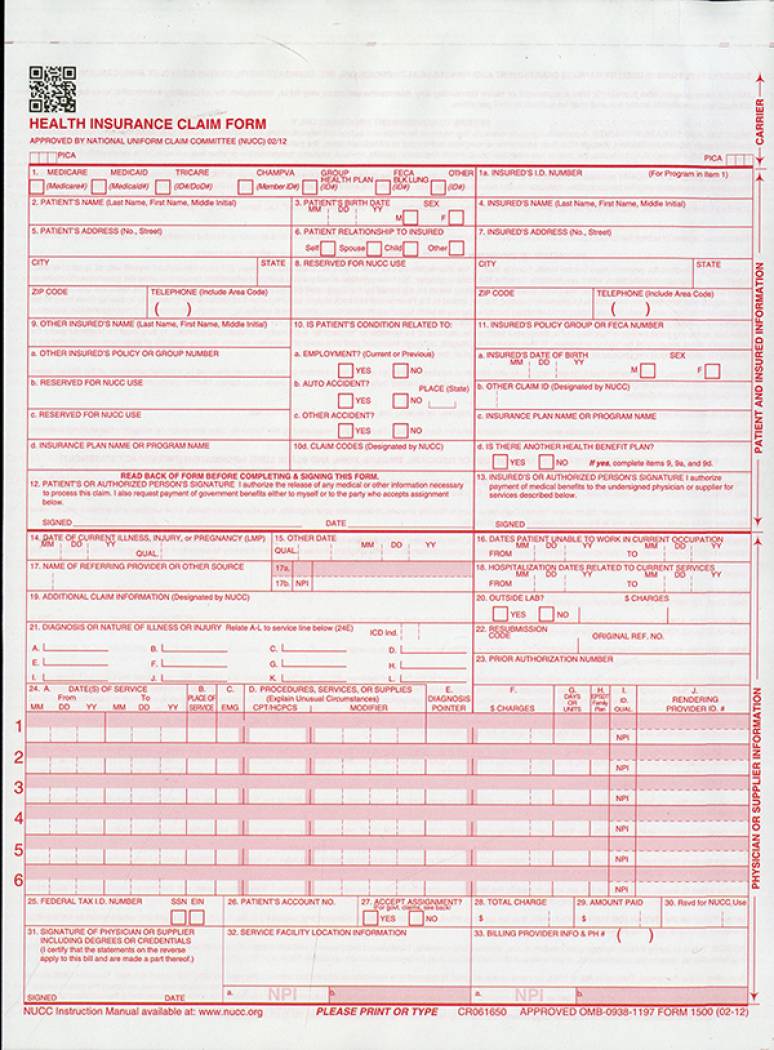
Updated 05182015 CMS-1500 02-12 Claim Form Instructions pv11182014 4 Shaded CMS-1500 02-12 field requirements The CMS-1500 02-12 claim form is shown below with Nevada Medicaid Required fields shaded red Situational fields shaded blue and Recommended fields shaded green. CMS-1500 Claim Form Introduction Purpose The purpose of this module is to provide an overview of the CMS-1500 claim form. Updated versions of this instruction manual are released each July.
INSURANCE PLAN NAME. Mandatory blocks must be completed. CMS 1500 claim form - How to fill out correctly - Instruction.
The 1500 Claim Form instructions were initially approved by the NUCC in November 2005. Complete claim submission - some tips. The Form CMS-1500 02-12 has the ability to capture up to four modifiers.
The necessary fields outlined below for Medicare secondary payer MSP must be completed. Medicare Enrollment - question and answer part 2. A CMS 1500 with field descriptions and instructions.
The other insurance carrier. For a Medicare crossover claim or Medicare Replacement plan claim leave this field blank. CMS-1500 02-12 claim form instructions when Medicare is secondary.
Conditionally mandatory blocks must be completed if applicable. CMS 1500 Form Item Instructions Item 1 Type of Health Insurance Coverage Applicable to the Claim Show the type of health insurance coverage applicable to this claim by checking the appropriate box eg if a Medicare claim is being filed check the Medicare box. Referring provider Ordering provider and billing provider - CMS 1500 UB04 form FAQ.
Therefore the instructions have and will continue to evolve. 30 Situational For a claim with no coverage other than Medicaid enter the total from field 28. When applicable show HCPCS code modifiers with the HCPCS code.
Please do not write or type above block 1 of the claim form. CMS 1500 claim form - How to fill out correctly - Instruction Elective inpatient services Out-of-state ambulance transports Select medical equipment and supplies Select prosthetic and orthotic services Select vision services Transplant services. 60 Zeilen When a claim involves multiple referring ordering or supervising physicians use.
06022020 CMS-1500 Claim Form Instructions This document is intended to provide Alaska Medicaid-specific instructions and clarifications for completion of the 1500 claim form version 0212. Enter the patients date of birth in MMDDYY format and the patients sex. Instructions for Completing the CMS 1500 Claim Form The Center of Medicaid and Medicare Services CMS form 1500 must be used to bill SFHP for medical services.
It is to be used as a companion to and not a. Enter the procedures services or supplies using the CMS Healthcare Common Procedure Coding Systme HCPCS code. Centers for Medicare Medicaid Services.
CMS-1500 Claim Form Instructions Rev. This information can be used by AB MACs B to determine whether the Medicare patient has other coverage that must be billed prior to Medicare payment or whether. Enter one of the following qualifiers as appropriate to identify the role that this physician or non-physician practitioner is performing.
The form is used by Physicians and Allied Health Professionals to submit claims for medical services. Complete the items below on the CMS-1500 02-12 claim form or electronic equivalent in addition to all other claim form requirements when Medicare is the secondary payer. Medicare provider Enrollment question and answer part 1.
This module presents claim completion processing instructions and offers participants general billing information required by the Medi-Cal program. CMS-1500 0212 BILLING INSTRUCTIONS FOR APPLIED BEHAVIORAL ANALYSIS Locator Description Instructions Alerts 1 Medicare Medicaid Tricare Champus Champva Group Health Plan Feca Blk Lung Required -- Enter an X in the box marked MedicaidMedicaid. When a claim involves multiple referring ordering or supervising physicians use a separate CMS-1500 claim form for each ordering referring or supervising physician.
If more than four modifiers are needed use modifier 99 overflow as the fourth modifier and enter the. Enter the three digit carrier code and name of any other insurance the patient has. Cms-1500 pdf Home A federal government website managed and paid for by the US.
Item 1a Insureds ID Number Patients Medicare Health Insurance Claim Number - HICN. The NUCC continues to research the type of data that are typically reported as well as the required data elements that may apply to public and private payers. Please refer to the CMS 1500 Third-Party Liability Claim Instructions or CMS 1500 Medicare Crossover Instructions if applicable.
Enter the street city state and zip code of the patient. Do not put social security numbers on the claim form. Providers may use these instructions to complete this form.