The latest setup file that can be downloaded is 3 MB in size. This is a required field.
 Cms 1500 Paper Claim Small Png Fiachra Forms Charting Solutions
Cms 1500 Paper Claim Small Png Fiachra Forms Charting Solutions
Claims must be made within 12 months after services are provided.
Cms 1500 claim form download. PLEASE PRINT OR TYPE FORM HCFA-1500 12-90 FORM RRB-1500 FORM OWCP-1500 APPROVED OMB-0938-0008. 7500 Security Boulevard Baltimore MD 21244. The CMS -1500 PDF is ideal for submitting the standard paper claim to bill for services.
For complete instructions refer to Chapter 6 of the DME Supplier Manual located under Publications. BECAUSE THIS FORM IS USED BY VARIOUS GOVERNMENT AND PRIVATE HEALTH PROGRAMS SEE SEPARATE INSTRUCTIONS ISSUED BY APPLICABLE PROGRAMS. APPROVED OMB-093B-1197 FORM CMS-1500 06-15 OMB No.
I would like to be able to save versions of the file for different patients with their identifying information. CMS. PLEASE PRINT OR TYPE APPROVED OMB-0938-1197 FORM 1500 02-12 APPROVED OMB-0938-1197 FORM 1500 02-12 1a.
Family Planning and. Template for CMS 1500 claim. In this video Dan Kimball CEO of Fiachra Forms provides a step by step tutorial on how to download the fillable CMS 1500 PDF claim form from Fiachra Forms.
You can install this PC program on Windows XPVista 32-bit. DO NOT MAIL COMPLETED CLAIM FORMS TO THIS ADDRESS. The template could be for MS Word or for MS Excel.
Providers should carefully read the information in this manual concerning Family PACT ICD-10-CM diagnosis codes and documentation requirements. CMS-1500 ZIP Home A federal government website managed and paid for by the US. Commonly this programs installer has the following filename.
Any person who knowingly files a statement of claim containing any. Tips for completing the cms-1500 claim formfield field number description member. The NUCCs goal was to develop the NUCC Data Set NUCC-DS a standardized data set for use in an electronic.
INSUREDS NAME Last Name First Name Middle Initial 7. Download CMS Claim Form 1500 which is used by health care professionals to bill Medicare and Medicaid. The delay reason code indicates that the claim form is being submitted after the six month billing limit.
Family Planning-Related Services. Centers for Medicare Medicaid Services. Instructions for Completing OWCP-1500 Health Insurance Claim Form For Medical Services Provided Under the FEDERAL EMPLOYEES COMPENSATION ACT FECA the BLACK LUNG BENEFITS ACT BLBA and the ENERGY EMPLOYEES OCCUPATIONAL ILLNESS COMPENSATION PROGRAM.
Sample cms-1500 claim form for physician offices and free-standing clinicsdisclaimer. While Family PACT claims are generally billed with the same method as Medi-Cal claims there are some unique differences for Family PACT. I am looking for a template to complete CSM 1500 health insurance claim forms and print to a standard pre-printed single sheet CMS 1500 red claim.
In addition to Medicare parts AB and for Medicare durable medical equipment Administrative Contractors. CMS-1500 Software 15 can be downloaded from our software library for free. September 2020 Delay Reason Codes Claims can be billed beyond the six month billing limit if a delay reason code is used.
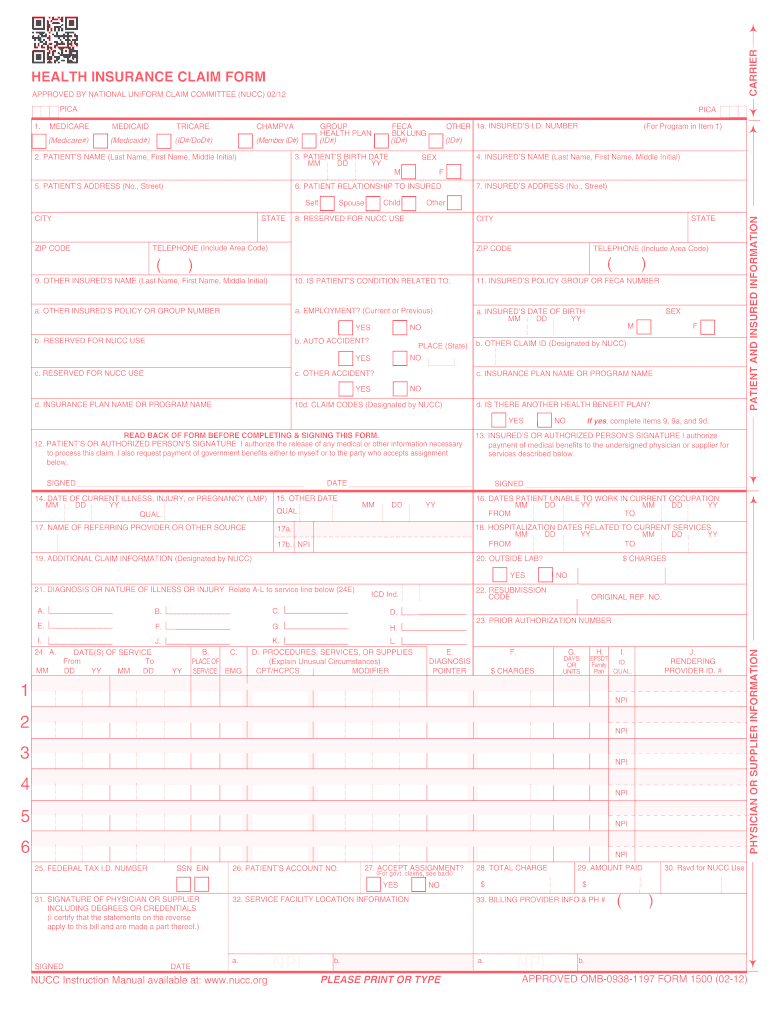
CMS-1500 CMS Form Number. Our free fillable CMS 1500 form PDF is a resource you can keep on hand for repeated use. CMS 1500 Claim Form Instructions Tool.
Our CMS 1500 form PDF downloadable is simple to use and comes as a blank CMS 1500 claim form PDF. Cms 1500 claim form worksheet. Enter the patients last name.
Enter the patients Medicare number whether Medicare is the primary or secondary payer. Cms 1500 form. Download Formdocs CMS-1500 for Windows to fill-in print and submit for reimbursement CMS 1500 0212 Medical Billing Claim forms.
Type Print Save a CMS-1500 with Adobe Reader software. This is not inclusive of all applicable codes that may be reported on a cms-1500 claim form. Although a delay reason code designates approved reason for late claim submission these exceptions also have time limits.
For Medicare claims check Medicare Item 1a. INSUREDS DATE OF BIRTH b. The Uniform Claim Form Task Force was replaced by the National Uniform Claim Committee NUCC in the mid 1990s.
INSUREDS POLICY GROUP OR FECA NUMBER a. Effort the 1500 Claim Form is accepted nationwide by most insurance entities as the standard claim formattending physician statement for submission of medical claims. Providers should document and code appropriately at all times1.
T his address is for comments andor suggestions only. Simply type in the form fields and print. To view instructions hover over each field.
NUMBER For Program in Item 1 4. Its easy to download and you can fill in the fields using the suggested resources above. Health Insurance Common Claims Form.
INSUREDS ADDRESS No Street CITY STATE ZIP CODE TELEPHONE Include Area Code 11. D CMS-1500 Claim Form 4 Page updated.
 Download Fillable Hcfa 1500 Claim Form Pdf Rtf Word Freedownloads Net Fillable Forms Templates Form
Download Fillable Hcfa 1500 Claim Form Pdf Rtf Word Freedownloads Net Fillable Forms Templates Form
 2012 2021 Form Cms 1500 Fill Online Printable Fillable Blank Pdffiller
2012 2021 Form Cms 1500 Fill Online Printable Fillable Blank Pdffiller
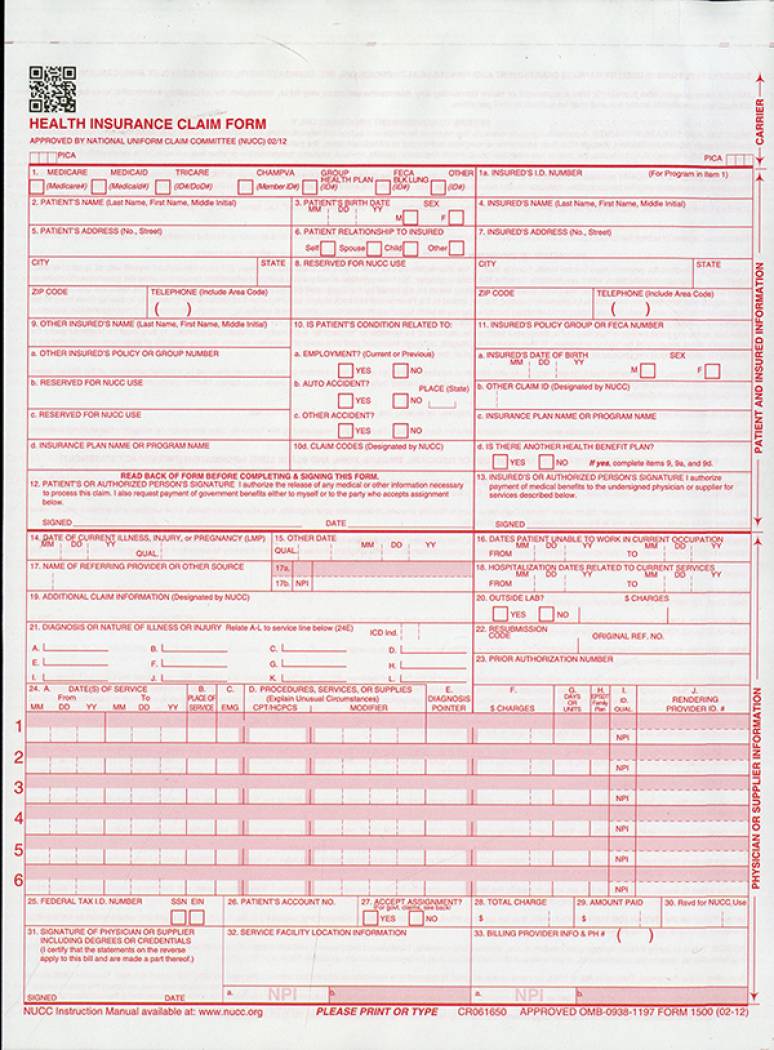
 1b Cms 1500 Insurance Claim Form Ver 02 12 Continuous Format 2 Part
1b Cms 1500 Insurance Claim Form Ver 02 12 Continuous Format 2 Part
 Cms 1500 Claim Form Pdf Free Download Unique Cms Form Templates Hcfa Best 1500 Claim Pdf Template Download Models Form Ideas
Cms 1500 Claim Form Pdf Free Download Unique Cms Form Templates Hcfa Best 1500 Claim Pdf Template Download Models Form Ideas
 Cms 1500 Free Download Create Edit Fill And Print Pdf Wondershare Pdfelement
Cms 1500 Free Download Create Edit Fill And Print Pdf Wondershare Pdfelement
Health Insurance Claim Form Picshealth
 1500 Claim Form Free S 9352 14 Cms 1500 Claim Forms Hcfa Version 02 12 1 Doctors Note Template Letter Example Cover Sheet Template
1500 Claim Form Free S 9352 14 Cms 1500 Claim Forms Hcfa Version 02 12 1 Doctors Note Template Letter Example Cover Sheet Template
 2012 2021 Form Cms 1500 Fill Online Printable Fillable Blank Pdffiller
2012 2021 Form Cms 1500 Fill Online Printable Fillable Blank Pdffiller
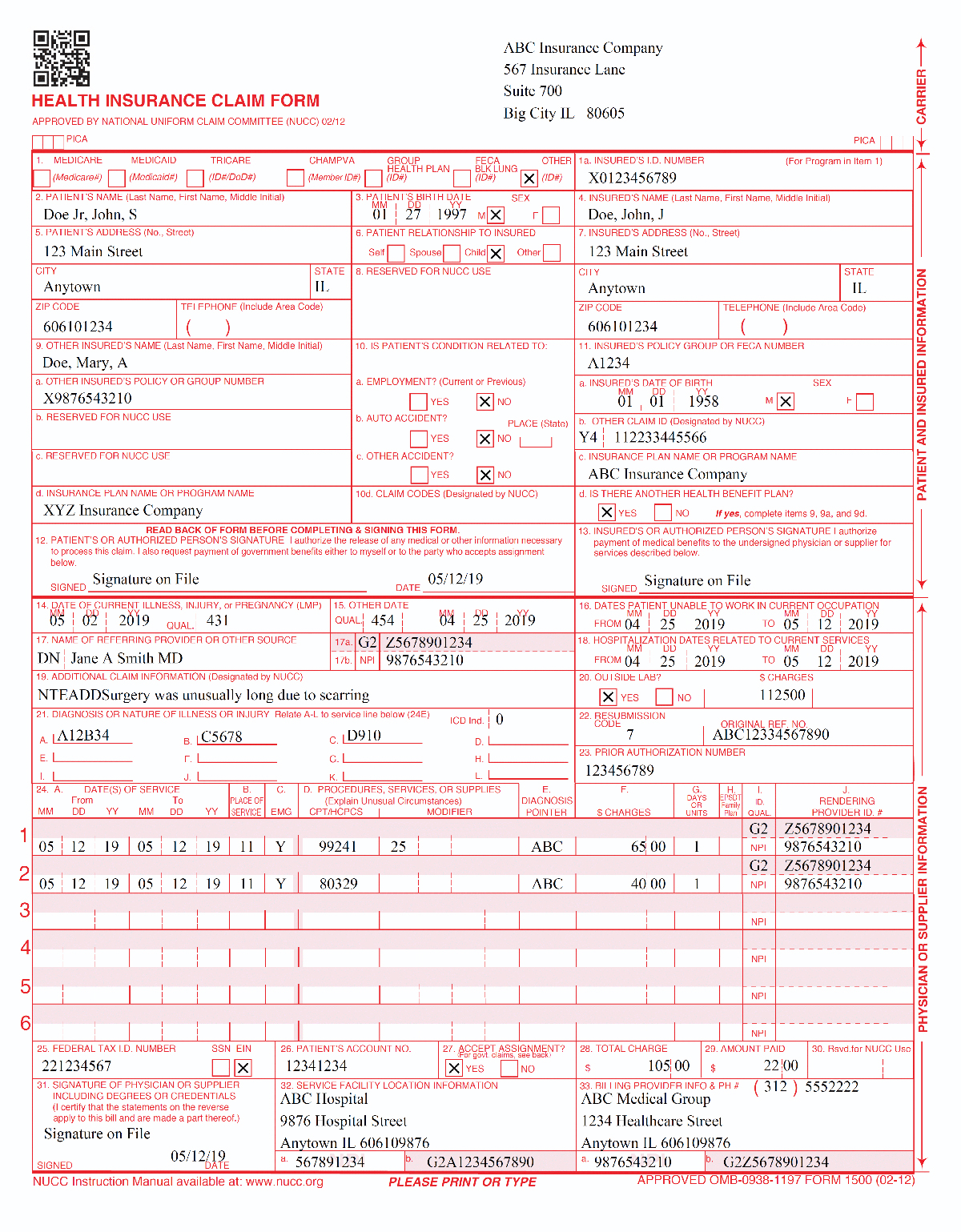
 Example Of Cms 1500 Form Completed With Cms 1500 Form Free Medical Coding Medical Billing And Coding Medical Billing Training
Example Of Cms 1500 Form Completed With Cms 1500 Form Free Medical Coding Medical Billing And Coding Medical Billing Training
 Medical Billing Process Cms 1500 Claim Form Billing Instruction
Medical Billing Process Cms 1500 Claim Form Billing Instruction
 Free Fillable Cms 1500 Template And Information Blue Summit Supplies
Free Fillable Cms 1500 Template And Information Blue Summit Supplies
 Mental Health Cms1500 Form Download Jpg Pdf
Mental Health Cms1500 Form Download Jpg Pdf
Https Www Cigna Com Static Www Cigna Com Docs Health Care Providers Form Cms1500 Pdf




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.