BCBS company AND also were enrolled in a BCBS health insurance or administrative services plan through your employer or other entity you must complete. This completed form together with the itemized bills should be submitted to.
 19 Printable Medical Claim Form Blue Cross Blue Shield Templates Fillable Samples In Pdf Word To Download Pdffiller
19 Printable Medical Claim Form Blue Cross Blue Shield Templates Fillable Samples In Pdf Word To Download Pdffiller
Please complete every item on claim form.
Bcbs medical claim form. Authorization - Complete for all claims. If you use a provider outside of the network you will need to complete and file a claim form for reimbursement. Sections B and C.
Even if you have medical vision dental or prescription drug coverage through Blue Cross Blue Shield of Michigan or Blue Care Network there may be occasions when you have to pay for services yourself. Claim Form to Pay InsuredSubscriber PO. BlueCross BlueShield of Tennessee Claims Service Center 1 Cameron Hill Circle Suite 0002 Chattanooga Tennessee 37402-0002.
When filing a Medicare Supplement claim follow these steps. Download the health benefits claim form. Use the Prescription Drug Mail Service Form.
Use this form to submit a health benefit claim for services that are covered under the Blue Cross and Blue Shield Service Benefit Plan. Otherwise you may skip to. Mail the completed claim form and attachments to.
MEDICAL EXPENSE CLAIM FILL OUT A SEPARATE FORM FOR EACH PATIENT. Blue Cross Blue Shield Settlement CO JND Legal Administration PO Box 91390. Forms and Documents Change Plan Forms Pharmacy Forms Payment Forms Enrollment Forms Claim Forms Appointment of Representative Form 2021 Drug Lists and Formularies Summary of Benefits Service Area Maps Low-Income Subsidy Premium Charts Health Plan Ratings Evidence of Coverage Protected Health Information.
Patients Name only one Patient per form. MEDICAL EXPENSE CLAIM FILL OUT A SEPARATE FORM FOR EACH PATIENT. Do NoT file this form if your Provider of Service is submitting these charges to Blue Cross and Blue Shield of Illinois.
Medical Transport Prior Approval Request. The beauty of Life is to plan strategically like fencing. If you filled out.
After your claim is processed well send you an Explanation of Benefits and a check if we owe you money. Submit a separate claim for each patient. Box 805107 Chicago Illinois 60680-4112.
Section A or Section C. Medicaid only BCCHP and MMAI Medicaid Service Authorization Dispute Resolution Request Form. To file a claim for 2019 coverage use this Prescription Drug Claim Form.
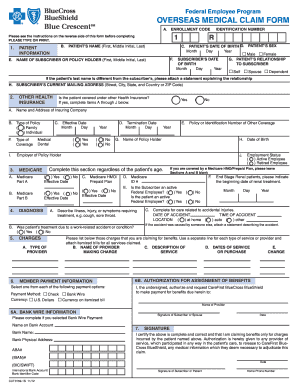
Contract Number as shown on your ID. MEDICAL CLAIM FORM Instructions for filing on second page PARTICIPANTS NAME Last First MI MEMBER ID NUMBER HOME ADDRESS Street City State Zip IS THIS A NEW ADDRESS. Overseas members should use the Overseas Medical Claim Form.
Form to identify the clinical justification for Intraoperative Neurophysiologic Monitoring. Do not file prescription drugs or dental claims with this form. Please print clearly with black ink or type.
1 InsuredSubscriber Name Last First Middle Initial Mailing Address City and State ZIP Code Insured Employed. Health Benefits Claim Form. Complete a separate claim form.
Medicaid Claims Inquiry or Dispute Request Form. Instructions for completion are listed on the reverse side. Complete a separate claim form for each covered family member.
Write your BlueCross BlueShield. ProviderDoctor Claim Inquiry Include this form when returning overpayments to Blue Cross NCStreamline claims processing by having members complete Provider Refund Return Form. Simply click on the form name to open them.
Post Service - Nerve Fiber Form Form to submit claims questions in writing. Use this form to file a claim for any eligible medical expenses when your physician or other provider does not file a claim. Non-Network Provider Written Direction of Payment Form.
Use this form to file a claim for any eligible medical expenses when your physician or other provider does not file a claim. Box 660044 Dallas Texas 75266-0044 Each item on this form needs to be completed. All claimants must complete.
Patients Name only one Patient per form 2. Forms to Download PDF format The forms below are all PDF documents. You must sign the claim form.
Blue Cross and Blue Shield of Illinois PO. Yes No PATIENTS NAME Last First MI MALE FEMALE DATE OF BIRTH MMDDYYYY RELATIONSHIP Self TO PARTICIPANT Spouse Child. Blue Cross provides you with comprehensive protection to meet challenges at ease.
In these cases use the Prescription Drug Claim Form. Important Notes When Completing the Claim Form. Planning is the Key to Success.
Medicaid only BCCHP and MMAI. Form Title Networks Expedited Pre-service Clinical Appeal Form. You must sign the claim form certification in Section F and mail it to the address below postmarked by November 5 2021 in order for your claim to be considered.
Type or use blue or black ink to complete. With this benefit you can order up to a 90-day supply of your prescriptions. All bills and Notification Forms should be marked with Policy Number and Insured Person Number and should be sent directly to Blue Cross Asia-Pacific Insurance Limited at 29th Floor BEA Tower Millennium City 5 418 Kwun Tong Road Kwun Tong Kowloon Hong Kong.
Section E regarding payment election. Originals of Bills only are acceptable. Durable Medical Equipment Certification Form.
If you regularly take medication you may also want to look into our mail-order service. Please print clearly with black ink or type. Of this claim form.
If you recently visited a doctor outside of your network and you need to submit a claim you can use one of these claim forms.















/ScreenShot2021-02-08at3.59.40PM-9f028cea3cb545d19e4c64e10ca68a06.png)