Your ID code is a combination of your day of. For compound drugs to be considered for reimbursement by the plan each ingredient of the compound must be found and payable in our claims system.
 Blue Cross Blue Shield Claims Form Fill Out And Sign Printable Pdf Template Signnow
Blue Cross Blue Shield Claims Form Fill Out And Sign Printable Pdf Template Signnow
Reimbursement may be considered taxable income so consult your tax advisor.
Blue cross blue shield reimbursement form. With this benefit you can order up to a 90-day supply of your prescriptions. Get your wellness reimbursement. Blue Cross Blue Shield of Massachusetts will make a reimbursement decision within 30 calendar days of receiving a completed request form.
If you regularly take medication you may also want to look into our mail-order service. Sometimes the form is called Member Application for Payment Consideration which is the same as a claim form. Member Reimbursement Usually we pay your health care providers for you without you having to do anything.
You must sign the claim form certification in Section F and mail it to the address below postmarked by November 5 2021 in order for your claim to be considered. Use the form to keep track of eye doctor visits and test results. If you have any questions call 1-888-706-2583 weekdays from 8 am.
Click on Claim Forms and choose the form preferred For more information and to confirm your coverage please call Customer Service. Products and services are provided by Horizon Blue Cross Blue Shield of New Jersey Horizon Insurance Company Horizon Healthcare of New Jersey Braven Health andor Horizon Healthcare Dental Inc each an independent licensee. Eyeglasses Reimbursement This form is only for ABP Medicaid Expansion Population members who are 21 years and older and have diabetes andor high blood pressure.
You will need your 4-digit ID code. If you were on a cruise youll use the same claim form for reimbursement. Just choose the form based on your group or plan and the service.
To file a claim for 2019 coverage use this Prescription Drug Claim Form. Blue Essentials SM Blue Advantage HMO SM and Blue Premier SM. Use this form to.
Blue Medicare Supplement Insurance SM Plan. This form is how you ask us to reimburse you. Letter prefix 2 digits following members name see ID card Patients Last Name.
Any missing or incomplete information may result in delay of payment or the form being returned. Blue Cross Blue Shield Settlement CO JND Legal Administration PO Box 91390. Out-of-Network Provider Negotiation Request Form.
Available with these plans. Blue Cross MedicareRx PDP SM Plan Documents. Member Reimbursement Oral Enteral Food Products Form Complete and submit this form to request reimbursement.
Use the Prescription Drug Mail Service Form. You can use these claim forms to ask us for reimbursement. Youll go to a page that explains the form and has a link to download it.
Please enter the subscriber number from your ID card. Find Medicare Advantage Plan Medicare Advantage Dual Care Plan HMO SNP Prescription Drug Plan and Medicare Supplement Insurance Plan forms and documents you need to help you manage your Medicare plan. Please fully complete the form print clearly.
Renewal Audit Package You and your dependents must live in Massachusetts to renew your individual health plan with Blue Cross Blue Shield of MA. A form authorizing Blue Cross Blue Shield of Massachusetts to send specific information to a specific individual. Use the links below to printview copies of our most frequently used forms.
In-network providers will need to enter a password to access this section of the site. This section provides additional reimbursement details. Blue Cross Medicare Advantage SM Plans Documents.
To see all available Qualified Health Plan options go to the New Jersey Health Insurance Marketplace at Get Covered NJ. From your Blue Cross Blue Shield of Michigan member. Member Reimbursement Donor Egg and Sperm Complete and submit this form to request reimbursement.
Use this form to write down your doctor visit. Use your 200 wellness reimbursement toward your favorite healthy activities like fitness classes weight-loss programs sports lessons and golf as well as fitness equipment and athletic footwear. Reimbursement is sent to the members address on file with Blue Cross.
Nonparticipating providers use this form to initiate a negotiation with Horizon BCBSNJ for allowed chargesamounts related to an inadvertent or involuntary service per the NJ Out-of-Network Consumer Protection Transparency Cost Containment and Accountability Act. You have to pay the doctor or hospital yourself. BlueCHiP for Medicare Value HMO-POS HealthMate for Medicare PPO.
Section 1 Member information. Blue View VisionSM Reimbursement Form Please complete the following steps prior to submitting the claim form to Blue View Vision. Overseas members should use the Overseas Medical Claim Form.
Reimbursement is sent to the members address on file with Blue Cross. Your doctor must sign and date the form before you send it to BCBSNM. The Blue Cross and Blue Shield names and symbols are registered marks of the Blue Cross and Blue Shield Association.
If you use a provider outside of the network you will need to complete and file a claim form for reimbursement. Blue Cross Blue Shield of Massachusetts will make a reimbursement decision within 30 calendar days of receiving a completed request form. Eastern time excluding holidays.
Health Benefits Claim Form. Register for your Medicare Reimbursement Account online.
 24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
 Blue Cross Blue Shield Overseas Claim Form Fill And Sign Printable Template Online Us Legal Forms
Blue Cross Blue Shield Overseas Claim Form Fill And Sign Printable Template Online Us Legal Forms
 24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
 Download Blue Cross Blue Shield International Medical Claim Form For Free Formtemplate
Download Blue Cross Blue Shield International Medical Claim Form For Free Formtemplate
 19 Printable Blue Cross Blue Shield Reimbursement Forms Templates Fillable Samples In Pdf Word To Download Pdffiller
19 Printable Blue Cross Blue Shield Reimbursement Forms Templates Fillable Samples In Pdf Word To Download Pdffiller
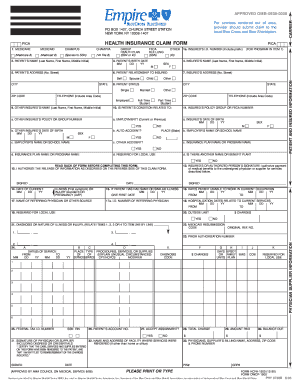
 Blue Cross Blue Shield Claim Form Fill Online Printable Fillable Blank Pdffiller
Blue Cross Blue Shield Claim Form Fill Online Printable Fillable Blank Pdffiller
 21 Printable Blue Cross Blue Shield Health Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
21 Printable Blue Cross Blue Shield Health Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
 19 Printable Medical Claim Form Blue Cross Blue Shield Templates Fillable Samples In Pdf Word To Download Pdffiller
19 Printable Medical Claim Form Blue Cross Blue Shield Templates Fillable Samples In Pdf Word To Download Pdffiller
Blue Cross Blue Shield International Fillable Claim Form Fill Online Printable Fillable Blank Pdffiller
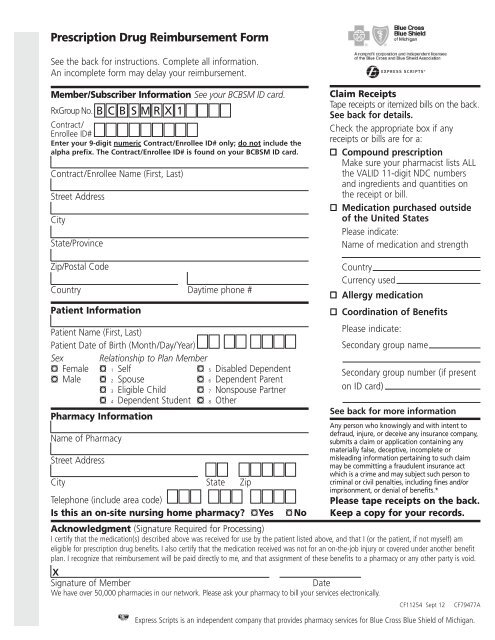 Rx Group Number Bcbsmrx1 Reimbursement Form Blue Cross
Rx Group Number Bcbsmrx1 Reimbursement Form Blue Cross
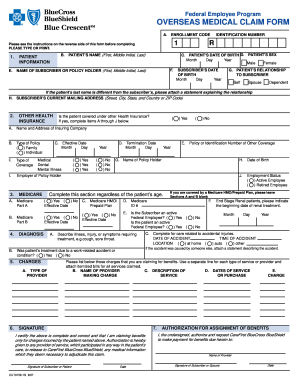 Blue Cross Blue Shield Overseas Medical Claim Form Fill Out And Sign Printable Pdf Template Signnow
Blue Cross Blue Shield Overseas Medical Claim Form Fill Out And Sign Printable Pdf Template Signnow
 Blue Cross Blue Shield International Medical Claim Form Pdfsimpli
Blue Cross Blue Shield International Medical Claim Form Pdfsimpli
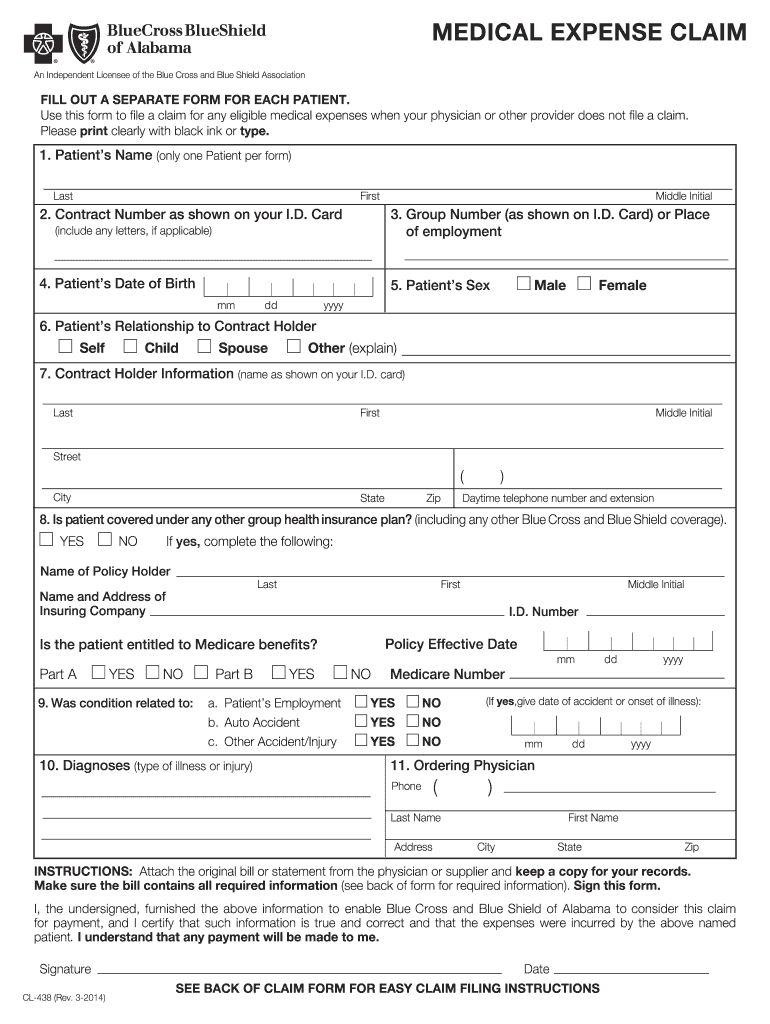 Blue Cross Blue Shield Of Alabama Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
Blue Cross Blue Shield Of Alabama Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
 21 Printable Blue Cross Blue Shield Health Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
21 Printable Blue Cross Blue Shield Health Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.