Residential Board and Care forms. AUTHORIZATION FOR RELEASE OF PROTECTED HEALTH INFORMATION CDCR 7385 Rev.

We encourage you to request a copy of your records and review them before authorizing the release of the records to someone other than you.

Medical records release form california. This information is required to conform to CCR Title 22 regulations to ensure a continuum of care to the resident client or child. 1019 DEPARTMENT OF CORRECTIONS AND REHABILITATION Instructions Note. Choose Medical Record Request and follow the prompts.
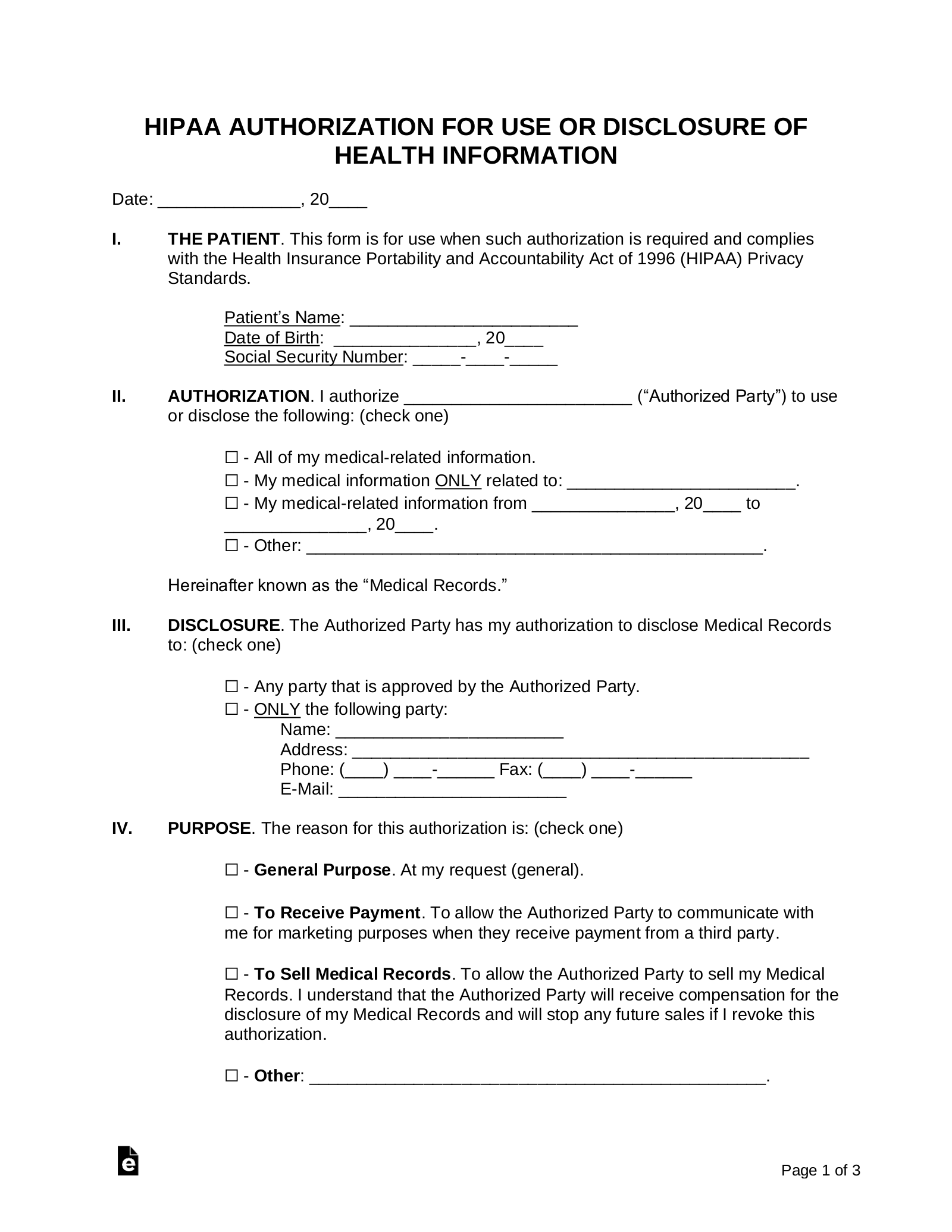
Your health anytime anywhere. If the authorization is not signed the information shall not be released except when required by law. _____ types in the PURPOSE section below q.
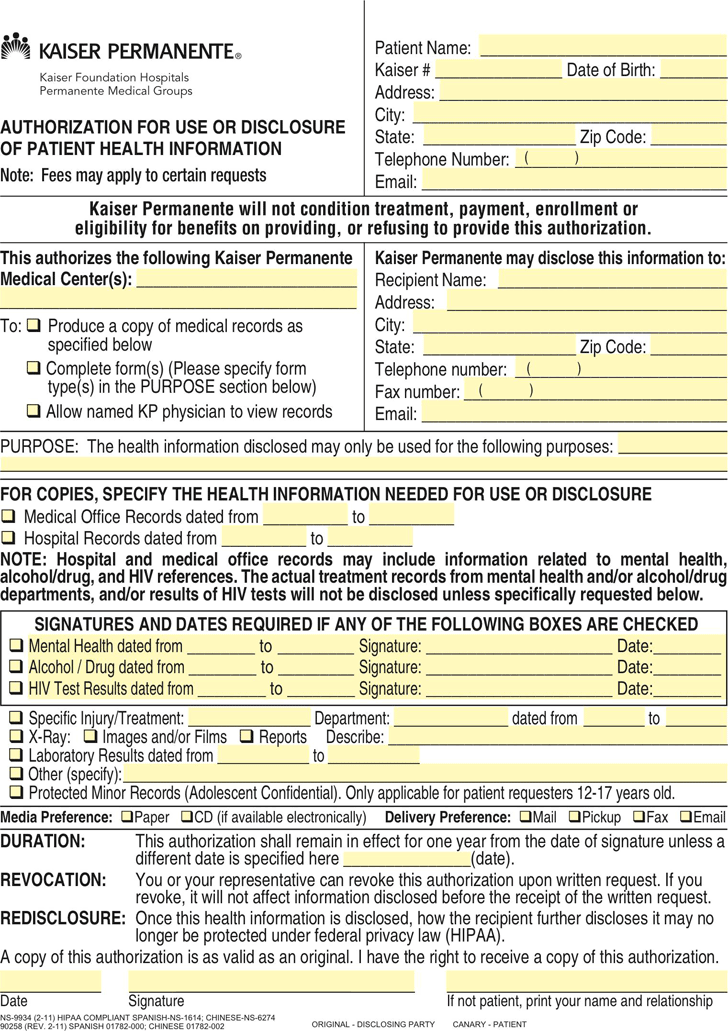
12 Sacramento CA 95817. DEPARTMENT OF HEALTH CARE SERVICES PRIVACY OFFICE. Produce a copy of medical records as specified below q.
The hospital shall not condition treatment or payment based on this authorization. Licensees should maintain a copy of this form in the facility records. Click Send us a customer service request.
Fill out the Request for Health Records form. Download and print the Authorization for Release of Health Information form below. Your records will be delivered to your MyChart account usually within three business days.
The health information disclosed may only be used for the following purposes. Allow named KP physician to view records PURPOSE. You can also mail the completed form to.
Complete forms Please specify form Telephone number. The person who authorized this release has a right to receive a copy of the release. Completed forms are returned to you rather than to a third party so you can review the information and make a copy for your records first.
The laws which authorize access to your records are available on the Internet and you might wish to review them for information about time lines a physician has to meet and the fees he or she may charge to provide the records. Autorización para la Divulgación de Información Médica - Spanish. Choose Health Medical Records.
Paper Copies of Medical Records. Complete and sign the form. For access to all portions of your medical record for any Sanford Health facility a written request should be sent to the Sanford Health Release of Information Department.
Authorization for Release of Information to a third-Party a Non-UCLA Provider Insurance Company Attorney etc Authorization for Release of Health Information - English. FOR COPIES SPECIFY THE HEALTH INFORMATION NEEDED FOR USE OR DISCLOSURE. OR Only the following records or types of health information including any dates.
You can submit a paper request by mail or fax. After you submit the form your requested records will be available in My CS-Link within five to seven days. Department of Motor Vehicles.
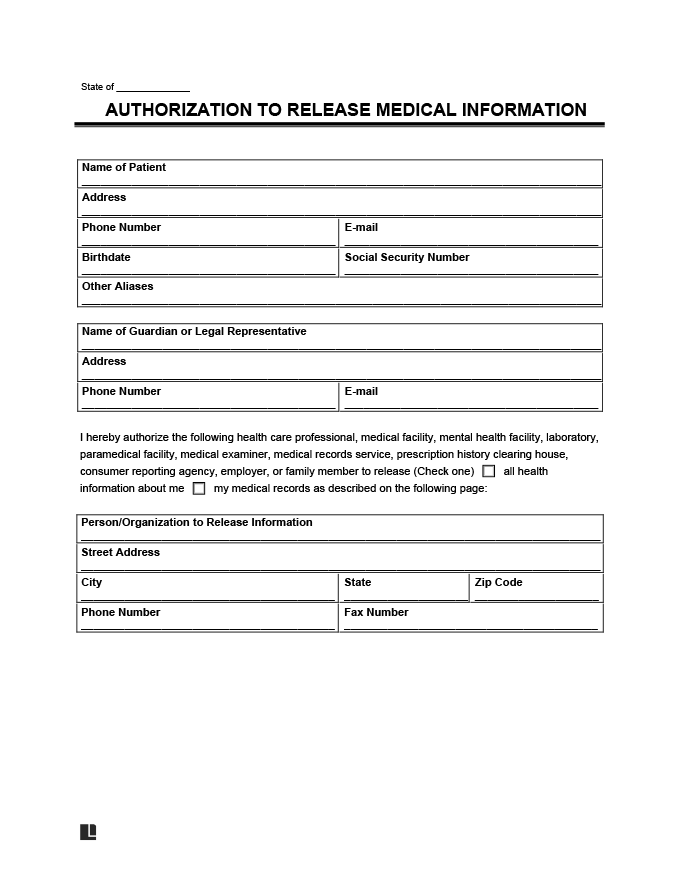
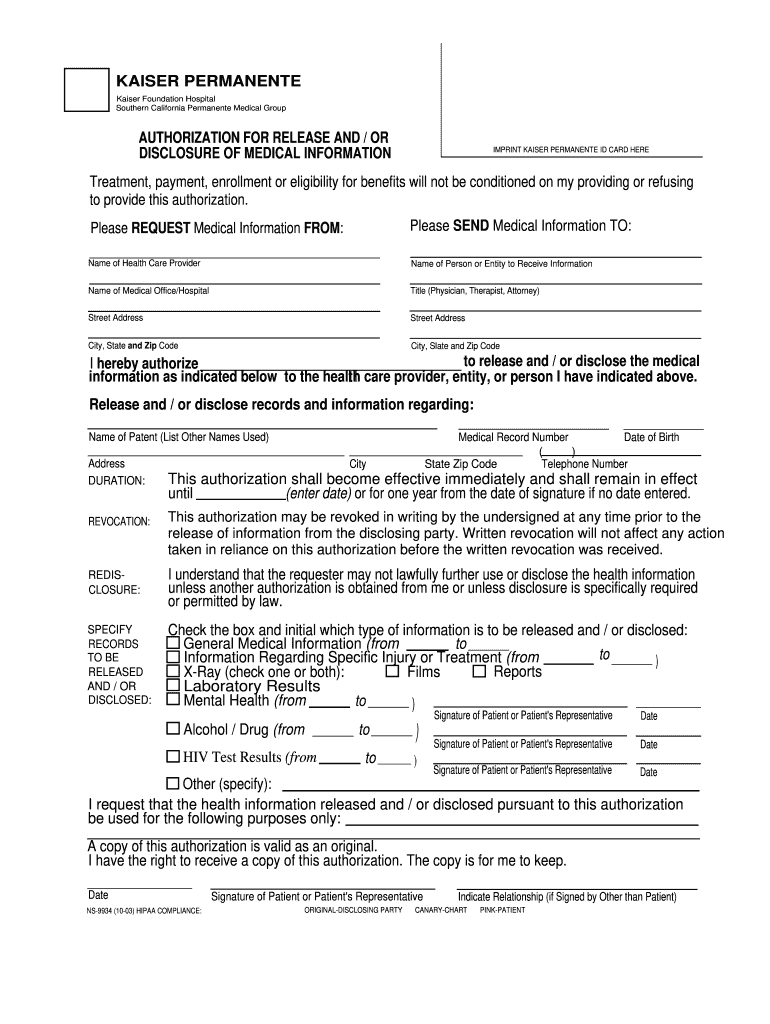
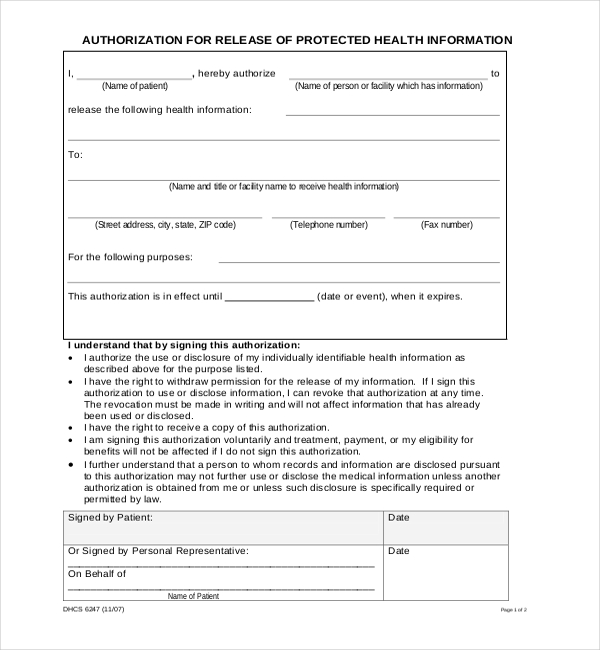
If you need copies of your health information for your own personal use or to forward to a health care provider or organization Kaiser Permanentes Release of Medical Information Departments are here to help you. I Name of patient hereby authorize Name of person or facility which has information to. Please read each section carefully and complete the required sections before signing.
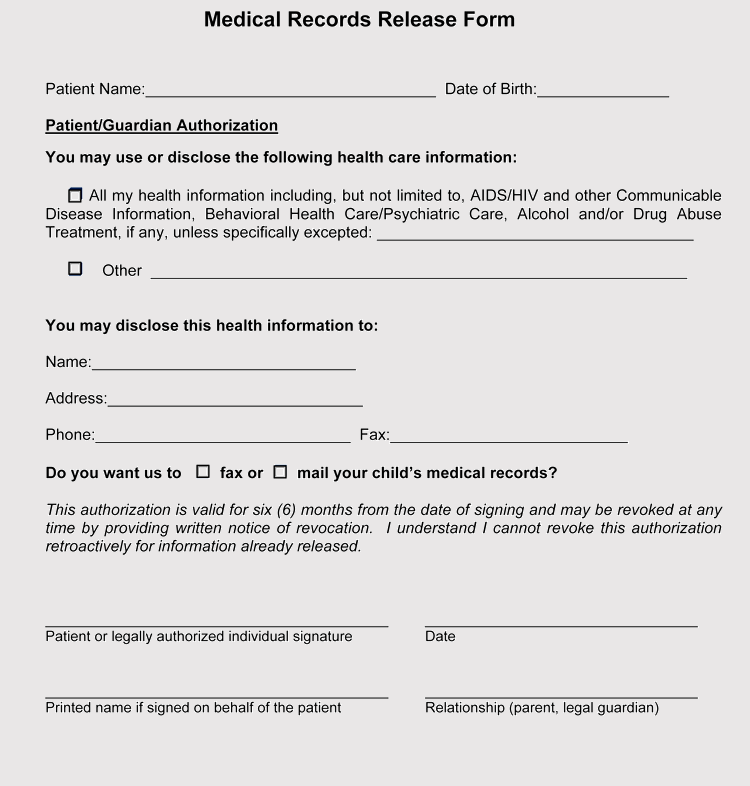
You can make a written request to either review or obtain a copy of your medical records pursuant to Health and Safety Code sections 123100 through 1231495. AUTHORIZATION FOR RELEASE OF PROTECTED HEALTH INFORMATION. Judicial Council of California wwwcourtscagov JV-226 Page 1 of 3 Revised July 1 2013 Optional Form JV-226 Authorization to Release Health and Mental Health Information I am the This form authorizes the release of the childs health andor mental health records to.
When you complete and sign this form health information about you will be released as you describe in the form. List the information released per this authorization on the back of this form. Submit the completed authorization form in person or mail to the appropriate Medical Records Department where you received your care and treatment.
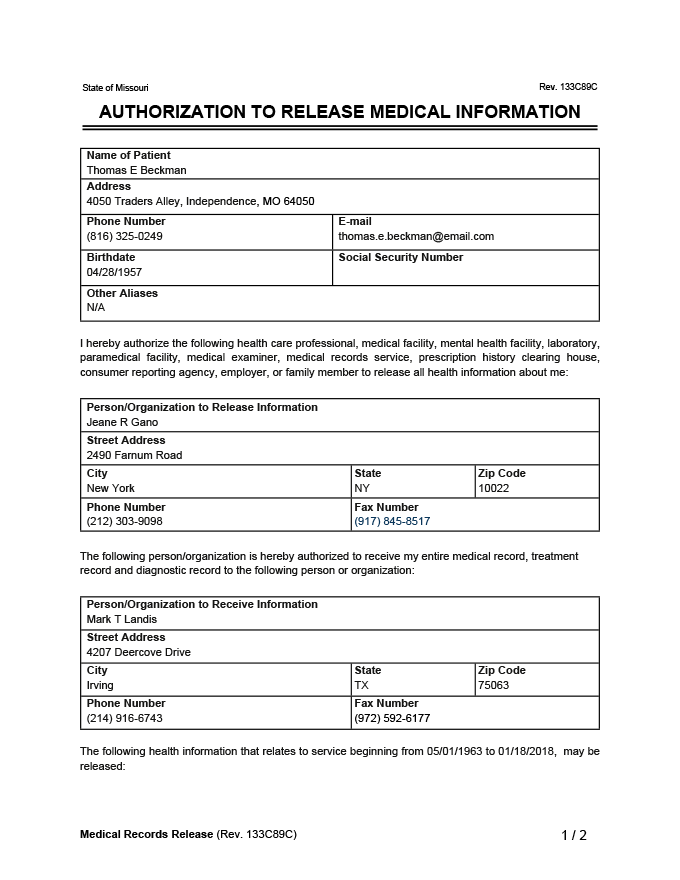
All health information pertaining to my medical history mental or physical condition and treatment received. If you have opted in for notification emails you will receive an email when your medical records are ready for download. Sanford Health offers secure online access to portions of your clinic medical record such as test results through My Sanford Chart.
If you have followed the requirements outlined in the Health Safety Code and the physician has not complied with your request you may file a complaint with the Medical Board. Part IV is the request for release of verbal health care information or health care information as part of written correspondence and Part V is the request for release of health care records. MedicalLegal Release of Information Unit 2315 Stockton Blvd Bldg.
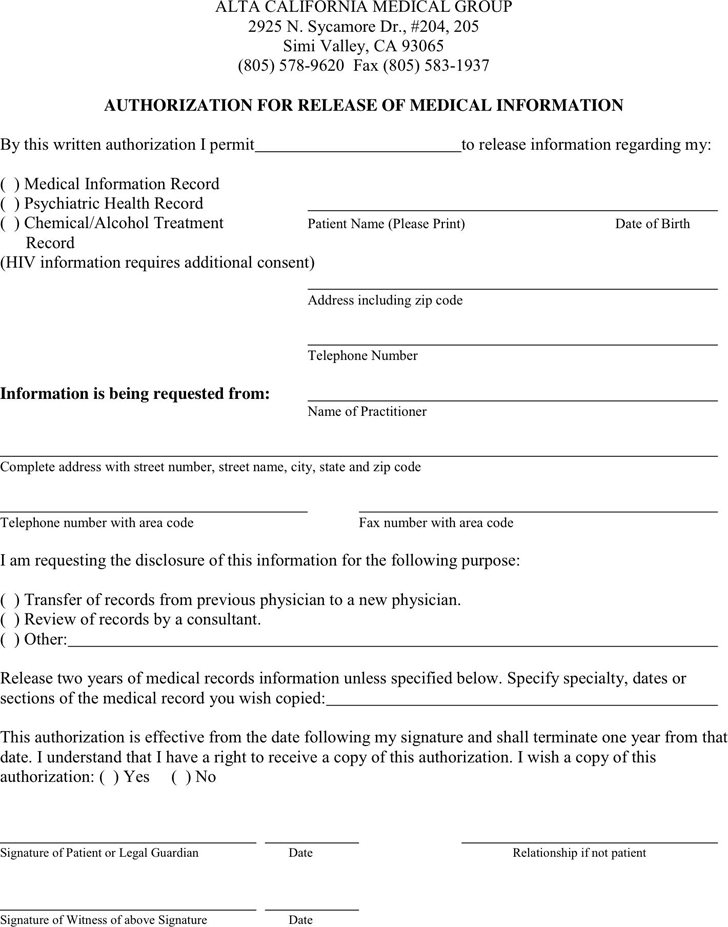
Working with your personal physicians office we can help you complete various forms regarding your health care including. Records that require a providers approval for release may take longer. Fax or mail the completed form to.
Release of Medical Information ROMI Manage your health information. Physicians will require a patient to sign a records release form to transfer records. Release the following health information.
If you are not currently a My Sanford Chart user learn more and sign up. Forms to verify illness or health condition. Fountain Valley CA 92708.
PersonsOrganizations authorized to receive the information Address street city state zip code The following information. Name and title or facility name to receive health information Street address city state ZIP code. The patient may refuse to sign the authorization.
Fillable Online Medical Records Request And Release Form California State Fax Email Print Pdffiller
 Download California Medical Records Release Form For Free Formtemplate
Download California Medical Records Release Form For Free Formtemplate
 Free Medical Records Release Authorization Form Hipaa Word Pdf Eforms
Free Medical Records Release Authorization Form Hipaa Word Pdf Eforms
 Medical Records Release Form Generic Request Template Pdf
Medical Records Release Form Generic Request Template Pdf
 Medical Records Release Template Free Template Download Customize And Print
Medical Records Release Template Free Template Download Customize And Print
 Kaiser Medical Records Release Form California Fill Online Printable Fillable Blank Pdffiller
Kaiser Medical Records Release Form California Fill Online Printable Fillable Blank Pdffiller
 40 Free Medical Record Release Forms Word Pdf
40 Free Medical Record Release Forms Word Pdf
![]() Kaiser Medical Records Release Form California New Medical Record Release Form Templates Blank Recordsase Template Models Form Ideas
Kaiser Medical Records Release Form California New Medical Record Release Form Templates Blank Recordsase Template Models Form Ideas
 Generic Medical Release Form Pdf Fill Out And Sign Printable Pdf Template Signnow
Generic Medical Release Form Pdf Fill Out And Sign Printable Pdf Template Signnow
Https Www Cahealthwellness Com Content Dam Centene Cahealthwellness Pdfs Chw Medical Records Release Eng 060717 Pdf
 Free 21 Sample Medical Records Release Forms In Pdf Word Excel
Free 21 Sample Medical Records Release Forms In Pdf Word Excel
 Medical Records Release Form Generic Request Template Pdf
Medical Records Release Form Generic Request Template Pdf
 Medical Records Release Template Free Template Download Customize And Print
Medical Records Release Template Free Template Download Customize And Print





No comments:
Post a Comment
Note: Only a member of this blog may post a comment.